This year in the Willamette Valley cases of respiratory illness among infants and children are skyrocketing. Many infants are experiencing illnesses which don’t usually peak until January.
You can protect your baby from RSV and other respiratory illnesses.
First though, what is RSV?
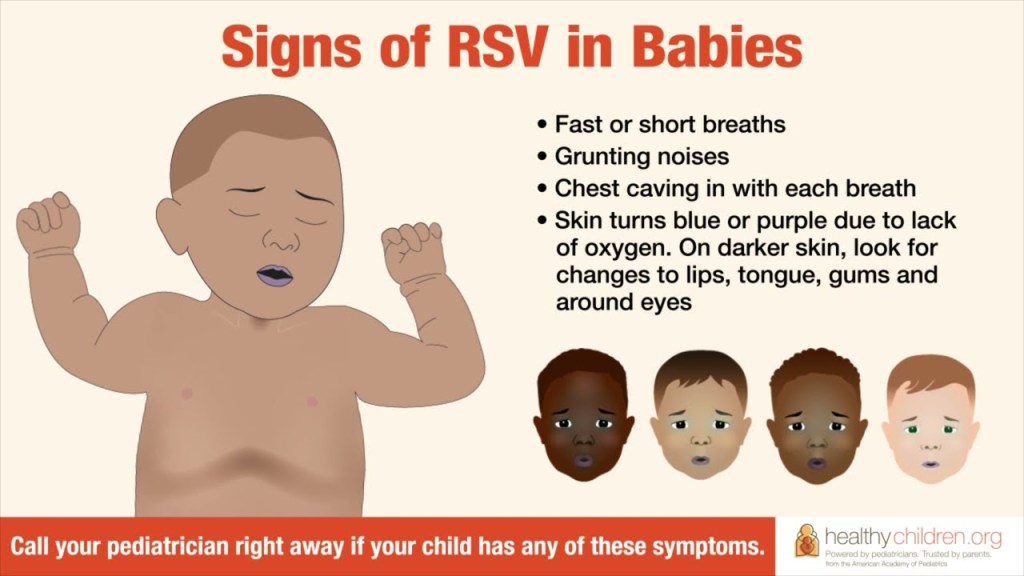
Respiratory syncytial (sin-Sish-uhl) virus, or RSV, is common respiratory virus which is generally mild but can be very dangerous for infants and the elderly. It typically causes mild, cold-like symptoms. RSV can be serious and is one of the top reasons for hospital admissions in the Fall and Winter for infants.
There are steps you can take to protect your baby, including:
Limiting visitors and people who touch and hold your baby. Adults can be contagious up to 24hrs before symptoms arise.
Hand washing and keeping people are sick, even mildly away form baby.
Tell family, friends, and even strangers not to kiss your baby.
Wear a mask in public and avoid contact in crowded places with limited air flow.
Breastfeed, ideally exclusively, for at least 6 months
“Conclusion: Breastfeeding has been shown to have a protective effect for infants with RSV bronchiolitis. WHO recommends minimum 6 months of exclusive breastfeeding for maximal immune protection against viral infections in infants.” Minerva, G. & Phillip, R. 2022. Impact of Breastfeeding on the Incidence and Severity of RSV Bronchiolitis in Infants: Systematic Review. Pediatrics
It can be confusing to figure out because some symptoms of food allergies/intolerance are also found with other types of feeding problems.
So how do you know for sure if your baby has an allergy?
Some symptoms are clearly associated with allergies and intolerance, not just a feeding problem. Babies will generally have more than one of these symptoms.
Wheezing or asthma
Congestion
Eczema or Hives
Diaper rash
Red eyes
Rash around the mouth
Unexplained stooling issues
Persistent mucous
Constipation
Diarrhea (without illness)
Food allergies mostly start after baby has started solids in addition to your milk. While food intolerances, can start at any time. Dairy is the most common in infants.
Other symptoms can go along with food allergies and intolerance butthey can also be a sign of another feeding problem.
Colic or discomfort Poor night time sleep Not napping Fussiness after feeds Temporary green stool Spit up or reflux Gassiness Blood in stool when you have nipple damage
How do you figure out the difference?
Schedule a consult with your IBCLC and they can do a full feeding assessment then refer you to a dietitian and an allergy specialist if a food allergy or intolerance is suspected.
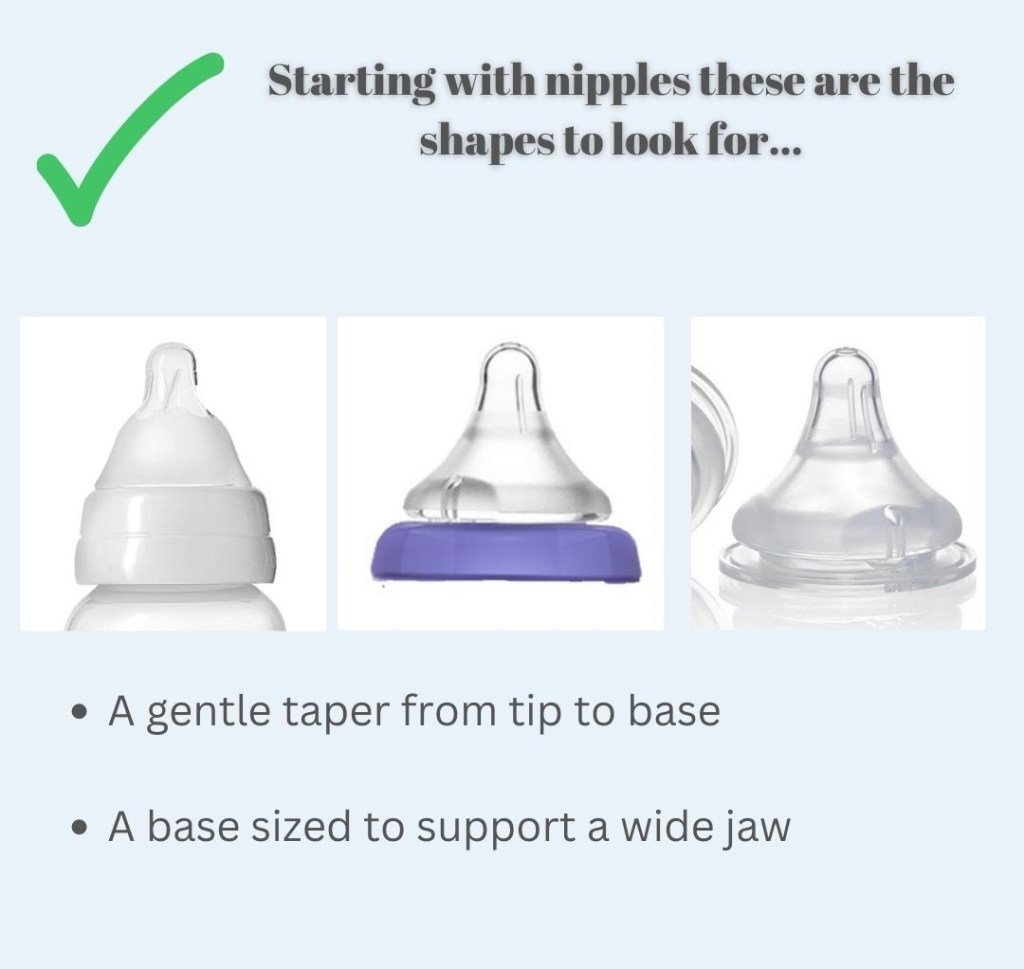
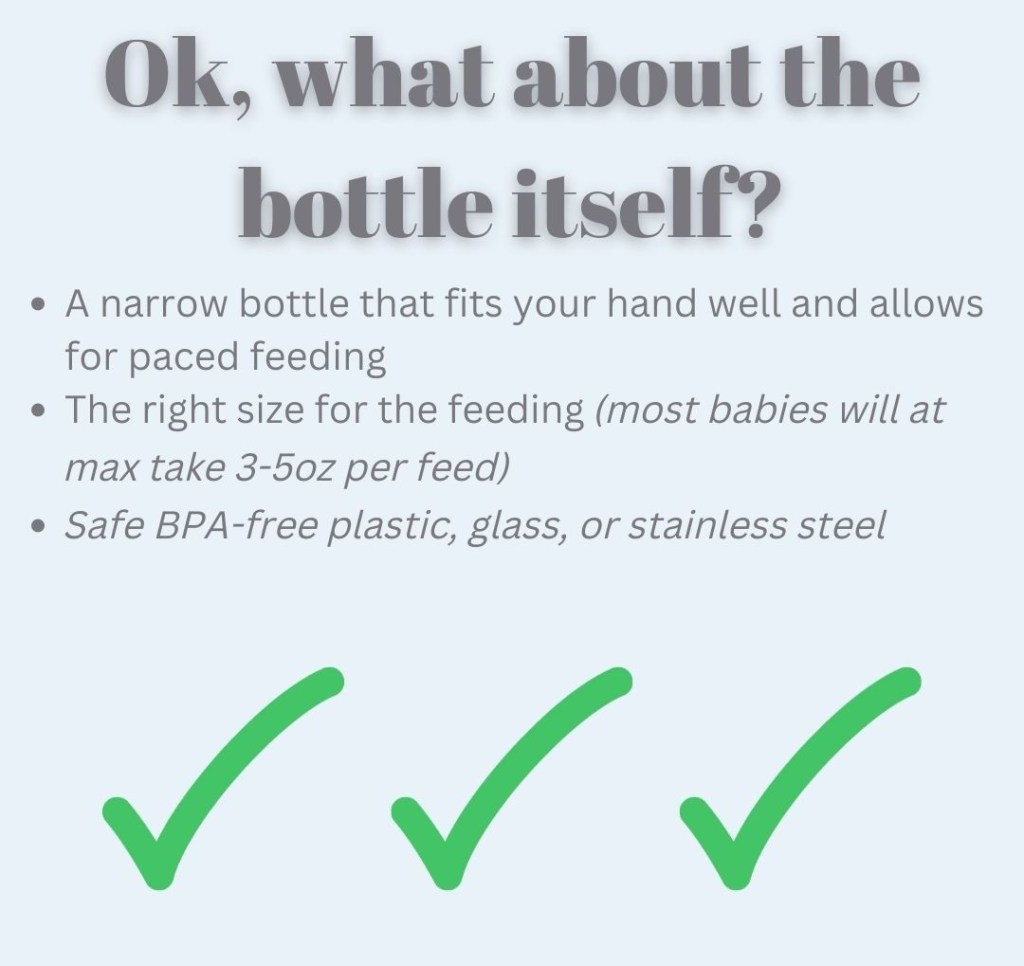
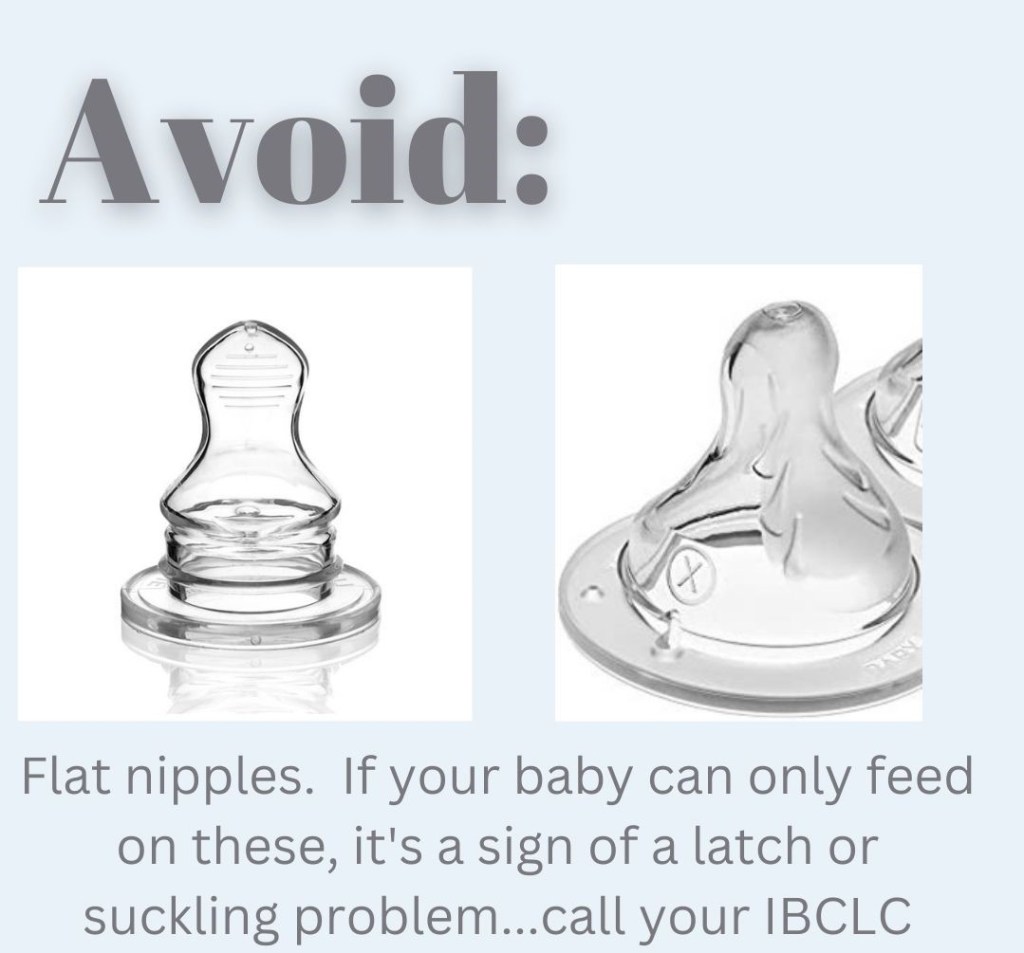
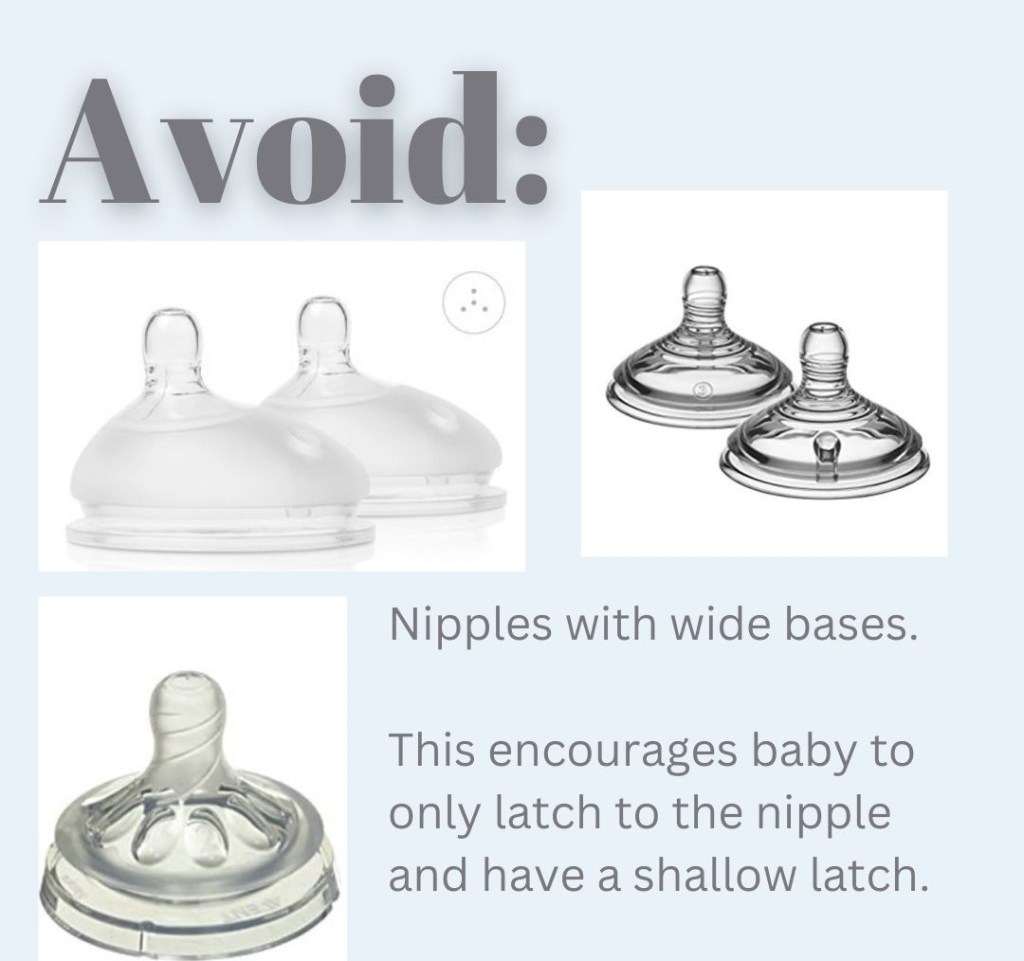
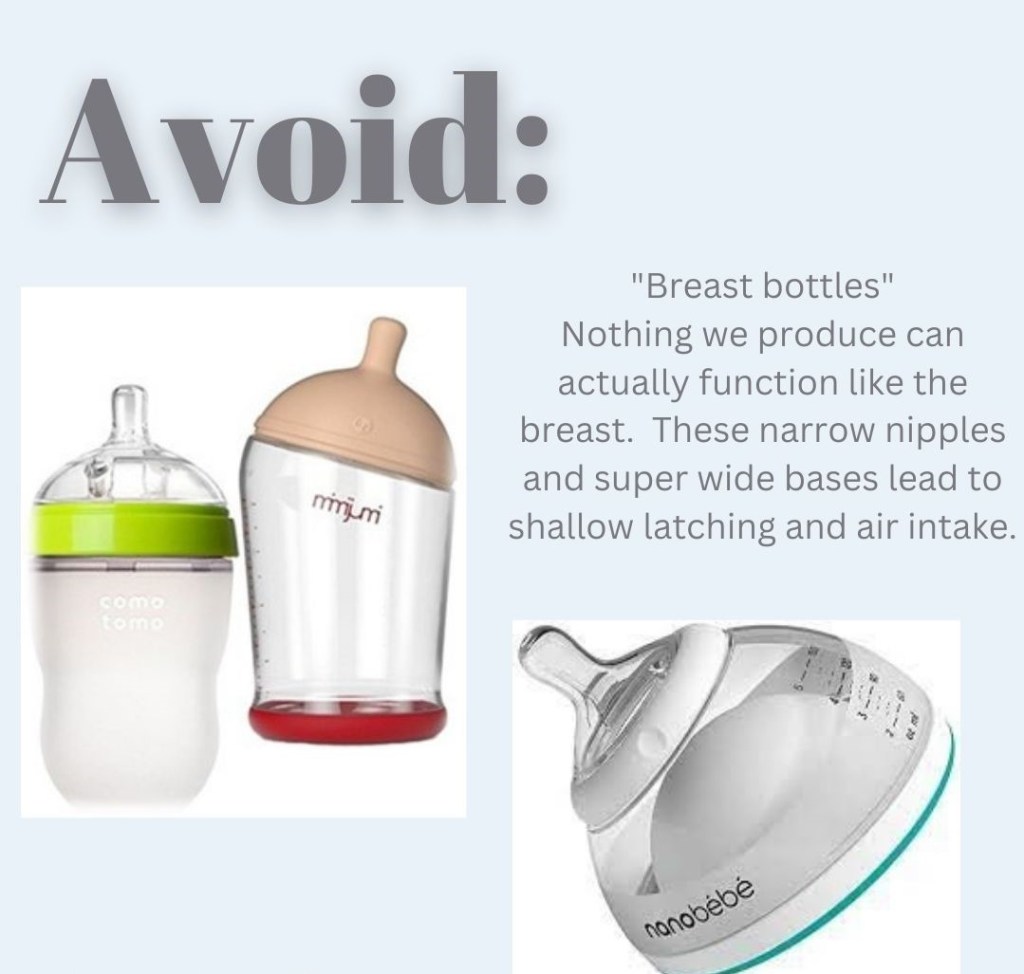
I’m returning to work soon. Which bottle should I pick for my baby?There are so many to pick from! How do I know which is right?Starting with nipples, these are the shapes to look for. A gentle taper from tip to base. A base sized to support a wide jaw. Ok, what about the bottle itself? A narrow bottle that fits your hand well and allows for paced feedings. The right size for the feeding (most babies will, at max, take 3-5oz per feed). Safe BPA-free plastic, glass, or stainless steel.AVOID: Flat nipples. If your baby can only feed on these, it’s a sign of a latch or suckling problem. Contact your IBCLC. AVOID: Nipples with a wide base. This encourages baby to only latch on the nipple and have a shallow latch.AVOID: “Breast bottles” Nothing we produce can actually function like the breast. These narrow nippels and super wide bases lead to shallow latching and air intake. Okay! We’ve narrowed it down!And the winners are…Evenflo Balance and Lansinoh Momma. Contact your IBCLC for help with bottle feeding.
There is a disproportionate incidence of diabetes among ethnic groups. Prevalence of diagnosed diabetes was highest among American Indians/Alaska Natives (14.7%), people of Hispanic origin (12.5%), and non-Hispanic blacks (11.7%), followed by non-Hispanic Asians (9.2%) and non-Hispanic whites (7.5%).
However, insulin resistance plays an important role in the physiological barriers to successful feeding as well as the perception or expectation of failure.
PCOS is a syndrome and the combination of symptoms is unique in each case, making identification more challenging. Many people never receive a formal diagnosis.
Symptoms can include:
•Raised levels of insulin (that can lead to excessive weight gain) •Raised levels of androgens hormones (that can lead to acne and growth of unwanted hair) •Irregular menses, ovarian cysts •Increased risk of developing diabetes •Underdevelopment of breast glandular tissue – not size
Medical conditions related to insulin resistance create additional challenges to lactation. Insulin resistance may delay Lactogenesis II – which is the milk transition from colostrum to mature milk and copious volume increase – this may be delayed by up to a week.
Some people with IR may never make enough milk to meet all the needs of their infant because of the role insulin plays in milk production and glandular growth during pregnancy, however, we do not know in advance that a person with diabetes will have insufficient supply.
Our focus should be on best practices to support these parents in the optimal outcomes for milk production and healthy infant feeding. We can do this by supporting nutrition which does not focus on weight alone, through offering medication therapy if indicated during pregnancy, by increasing access to lactation care both in-patient and after discharge, and increasing access to human donor milk for supplementation.
As providers we can also learn more about non-medication supports for managing milk supply which can include:
• Frequent milk removal using hands-on techniques • Learning about which herbs to use or avoid • Avoiding pacifiers and bottles, instead focusing on skin-to-skin and using at breast supplement tools • The use of donor milk until milk production is established • Frequent visits with an IBCLC in the first week after delivery • Supporting in-home care • Using Peer Support programs to encourage parents and monitor the need for medical intervention
With support, education, and provider support parents with PCOS can chestfeed successfully!
Manual therapies like chiropractic, osteopathic manipulation (these first 2 are most likely to be covered by your insurance), cranial sacral therapy (focuses on the head/neck/shoulders only), physiotherapy, and many more!
The practitioner and their skill set is an important factor in deciding which type to go with along with the areas your baby needs treated, your IBCLC or pediatrician should help you determine which will be right for your baby.
2. Oral motor exercises
These gentle exercises are meant to address compensations and work toward function. They are done in the mouth and on the face and may include other body movements. Unlike bodywork, these exercises are done daily by the parents as directed by your IBCLC. Some providers call this Suck Training.
3. Managing the feeding plan
This is evaluated and organized by your IBCLC. The feeding plan balances the need of the infant and parent and works toward feeding goals.
Your IBCLC will manage your feeding plan according to your goals and to get the bet outcomes for you. This can include counseling on pumping, feeding positions and techniques, supporting milk supply, and referring to other providers.
*these first 3 components are part of your pre and post release plan*
4. An effective release
Scissors or laser …it doesn’t matter as long as your provider is skilled and performs a full release to allow the tongue and/or other tissue to move normally. The release allows for movement while bodywork, oral motor training, and feeding plan management work together to get to normal function.
5. Wound care
Sometimes called stretches or exercises these are targeted on the site which was released (the diamond shape under the tongue). Wound care is necessary for posterior releases to prevent reattachment and aid in the tissue healing correctly.
Sometimes your provider will suggest oral motor exercises along with the wound care. Your IBCLC will suggest additional, customized oral motor training in addition to these.
Without all 5 components your baby may not achieve full functionality. Your IBCLC should be able to guide you through this process and make referrals to skilled providers as needed.
What to Expect After a Tongue Tie Release (Frenotomy)
When appropriate anesthetic is used, the procedure is generally not painful but it is irritating to be swaddled and have the mouth held open for the procedure. Your baby may be a little fussy after but can be soothed with skin-to-skin and a feeding.
Baby may initially feed very well but about 5-6 hours later they may be quite fussy and difficult to console. When adults get the procedure done, they report that they experience muscle fatigue which is quite uncomfortable. Try not to use a pacifier and instead to offer skin-to-skin and other forms of soothing. Smaller, closer spaced feeds may work better temporarily.
Work with baby’s skills and abilities. We aren’t trying to challenge their feeding during healing. Latch and hold your baby the way that works best for them.
Feeding starts to improve over time as the tongue strengthens and other muscles which have been compensating start to relax. The suck training exercises (oral motor work) recommended are very important in this process of “teaching” your baby how to use their newly released tongue and to address areas of tightness and weakness.
After about 4-5 days the wound will start to contract and feel tight again. Many parents worry that this is reattachment. Continuing your gentle wound care is important to keep these tissues soft.
Stretches should be done quickly and gently. I don’t recommend doing them before feeds to avoid associations with feeding. If you practice the stretches on yourself and your baby before the procedure it will increase your confidence and skill.
Effective and comfortable feeding requires a lot more than just a tongue which can fully move and function. It also requires that baby isn’t experiencing pain or discomfort anywhere else. Bodywork helps baby find full function through gentle manipulations. This can include pediatric chiropractic, osteopathic manipulation, cranial sacral therapy, or other types of bodywork. Ask your provider or IBCLC for referrals to providers who are experienced working with infants.
At home, you can support your baby with movement, massage, and at-home care like Tummy Time.
A visit with your IBCLC about 2-5 days after the procedure is important to check on the wound healing and to adjust your suck training and bodywork instructions.
August 15-21 is Asian American Native Hawaiian and Pacific Islander Breastfeeding Week! This year’s theme is Telling Our Own Stories. Elevating Our Voices. Organized by the Asian & Pacific Islander Breastfeeding Task Force, the week is a great time to listen and learn from AANHPI families, community members, and lactation support providers; and celebrate and share resources.
August 16, at 1 p.m. E.T. join 1,000 Days and the National WIC Association for the next live panel discussion. This week’s topic is AANHPI Breastfeeding, moderated by Darlena Birch, with presenters Wendy Fung and Pauline Sakamoto.