




In honor of our Black parents, I’d like to share the following articles and resources:
The B.L.A.C.K. Course – A full-scope lactation and breastfeeding education course made by and for Black People and folks supporting Black breastfeeding.
Black History Month 2021 Toolkit
Melanated Mammary Atlas – The Melanated Mammary Atlas® is your portal to a world of images displaying mammary related conditions on Asian, Indigenous, Black and Brown folks.
Chocolate Milk: The Documentary – A film about the state of breastfeeding in Black America from The African American Breastfeeding Project.
Articles and blogs
THE HISTORY OF BLACK WOMEN & BREASTFEEDING
Breastfeeding As An Act Of Resistance For The Black Mother
Organizations Focused on Black Breastfeeding
African-American Breastfeeding Coalition of Oregon
Black Mothers’ Breastfeeding Association
Breastfeeding Sisters That Are Receiving Support (BSTARS)
Indiana Black Breastfeeding Association
National Association of Professional and Peer Lactation Supporters of Color (NAPPLSC)


Many medications are totally fine to take during lactation. Many meds won’t affect milk production and they won’t harm your baby!
Medications, prescription and over the counter, are processed through several steps which determine how much makes it into your milk and determines if it will affect your baby or the milk production process.
Let’s take a look at this process!
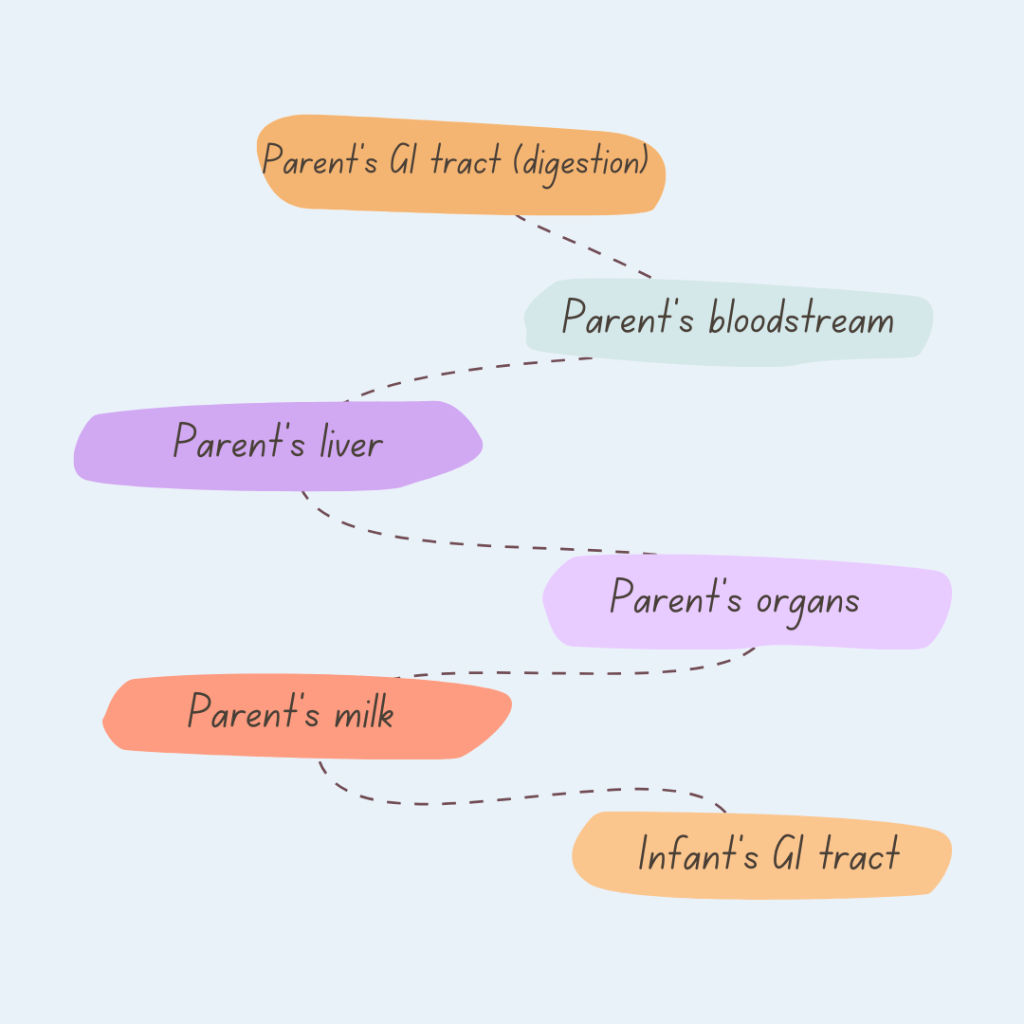
As you can see oral medications need to be digested, metabolized through the liver, processed through the target organs, before they can make it into the mammary tissue of the breast and into the milk.
If they make it that far the remaining molecules still have to be small enough and attracted to water, fat, or both to make it into the milk.
If it makes it into the milk it still needs to be digested and processed through baby’s liver before it will possibly affect baby!
Most medications are diluted to 0.5-10% of the parent’s dose before they even make it to baby! That’s very small!
There’s a lot that goes into determining if a medication is safe for you and baby during lactation. You can discuss the medications, supplements, and herbal remedies you are considering with your IBCLC who will provide you with resources to talk with your doctor.
Often there are alternatives if the medication you want to take is not compatible.
Since it’s cold and flu season you can check here for information about common medications you may be thinking of taking if you get symptoms.
The flu vaccine is safe to take while breastfeeding and gives your baby extra protection!

Life with a new baby is exciting and full of new experiences! But the holidays also bring chaos, lots of visits, travel, and stress. Which are the last things that new parents and babies need. When the holiday season rolls around, your family and friends will no doubt be thrilled to include your little one. How do you protect the peace and keep the boundaries for your family?
Here’s some ideas:
These conversations can be tough! Ask your partner and close friends to step in and help you navigate.

As many as 1 in 7 parents experience chronic low milk supply.
An estimated 5-15% of lactating parents experience CLMS (chronic low milk supply).
CLMS is associated with many common metabolic and endocrine conditions like:
Up to 20% of lactating parents may have PCOS

Many parents don’t know why they experience CLMS. There are significant Mental Health impacts from CLMS.
Experiencing CLMS may compound trauma and feelings of inadequacy from infertility, pregnancy, or birth challenges.
Connecting with other parents who have similar experiences and working with your IBCLC to make feeding comfortable and enjoyable can help.
Resources for support:
Wellmama http://www.wellmama.net 541-231-4343
Hope for Mothers Albany 541-812-4475 Lebanon 541-451-7872
Low Milk Supply Foundation https://lowmilksupply.org/
❤ Megan

It can be confusing to figure out because some symptoms of food allergies/intolerance are also found with other types of feeding problems.
So how do you know for sure if your baby has an allergy?
Some symptoms are clearly associated with allergies and intolerance, not just a feeding problem. Babies will generally have more than one of these symptoms.
Food allergies mostly start after baby has started solids in addition to your milk.
While food intolerances, can start at any time. Dairy is the most common in infants.
You only need to remove it from your diet for about 3 days to see a difference. You do need to remove all milk products though. Check this list so you can spot the dairy in the ingredients list.
Other symptoms can go along with food allergies and intolerance but they can also be a sign of another feeding problem.
Colic or discomfort
Poor night time sleep
Not napping
Fussiness after feeds
Temporary green stool
Spit up or reflux
Gassiness
Blood in stool when you have nipple damage
How do you figure out the difference?
Schedule a consult with your IBCLC and they can do a full feeding assessment then refer you to a dietitian and an allergy specialist if a food allergy or intolerance is suspected.
❤ Megan



We’ve talked about how PCOS and insulin resistance can affect lactation and milk production before but let’s explore this a bit more.

There is a disproportionate incidence of diabetes among ethnic groups.
Prevalence of diagnosed diabetes was highest among American Indians/Alaska Natives (14.7%), people of Hispanic origin (12.5%), and non-Hispanic blacks (11.7%), followed by non-Hispanic Asians (9.2%) and non-Hispanic whites (7.5%).
This, of course, is not the only disparity found in lactation among different ethnic groups.
However, insulin resistance plays an important role in the physiological barriers to successful feeding as well as the perception or expectation of failure.
PCOS is a syndrome and the combination of symptoms is unique in each case, making identification more challenging. Many people never receive a formal diagnosis.
Symptoms can include:
•Raised levels of insulin (that can lead to excessive weight gain)
•Raised levels of androgens hormones (that can lead to acne and growth of unwanted hair)
•Irregular menses, ovarian cysts
•Increased risk of developing diabetes
•Underdevelopment of breast glandular tissue – not size
Medical conditions related to insulin resistance create additional challenges to lactation. Insulin resistance may delay Lactogenesis II – which is the milk transition from colostrum to mature milk and copious volume increase – this may be delayed by up to a week.
Some people with IR may never make enough milk to meet all the needs of their infant because of the role insulin plays in milk production and glandular growth during pregnancy, however, we do not know in advance that a person with diabetes will have insufficient supply.
Our focus should be on best practices to support these parents in the optimal outcomes for milk production and healthy infant feeding. We can do this by supporting nutrition which does not focus on weight alone, through offering medication therapy if indicated during pregnancy, by increasing access to lactation care both in-patient and after discharge, and increasing access to human donor milk for supplementation.
As providers we can also learn more about non-medication supports for managing milk supply which can include:
• Frequent milk removal using hands-on techniques
• Learning about which herbs to use or avoid
• Avoiding pacifiers and bottles, instead focusing on skin-to-skin and using at breast supplement tools
• The use of donor milk until milk production is established
• Frequent visits with an IBCLC in the first week after delivery
• Supporting in-home care
• Using Peer Support programs to encourage parents and monitor the need for medical intervention
With support, education, and provider support parents with PCOS can chestfeed successfully!
❤ Megan
