




As many as 1 in 7 parents experience chronic low milk supply.
An estimated 5-15% of lactating parents experience CLMS (chronic low milk supply).
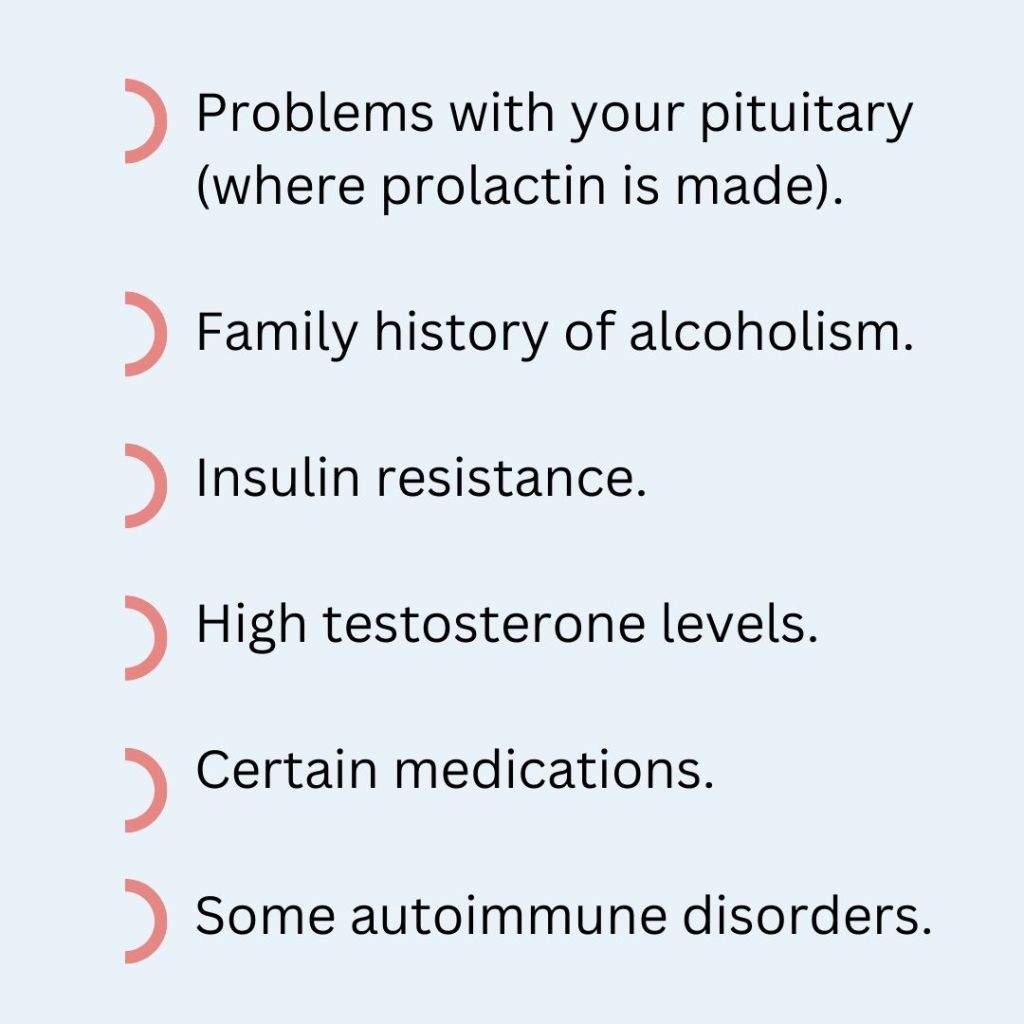
CLMS is associated with many common metabolic and endocrine conditions like:
Up to 20% of lactating parents may have PCOS

Many parents don’t know why they experience CLMS. There are significant Mental Health impacts from CLMS.
Experiencing CLMS may compound trauma and feelings of inadequacy from infertility, pregnancy, or birth challenges.
Connecting with other parents who have similar experiences and working with your IBCLC to make feeding comfortable and enjoyable can help.
Resources for support:
Wellmama http://www.wellmama.net 541-231-4343
Hope for Mothers Albany 541-812-4475 Lebanon 541-451-7872
Low Milk Supply Foundation https://lowmilksupply.org/
❤ Megan

❤ Megan





Does your baby gag, choke, and cough during feeding? Are they sputtering and tugging on your breast? Ever notice them clicking or leaking milk? What about gas…do they seem to have an awful of it?
There could be a number of things causing baby to struggle with feeding.
Let’s learn about the differences.

Strong MER
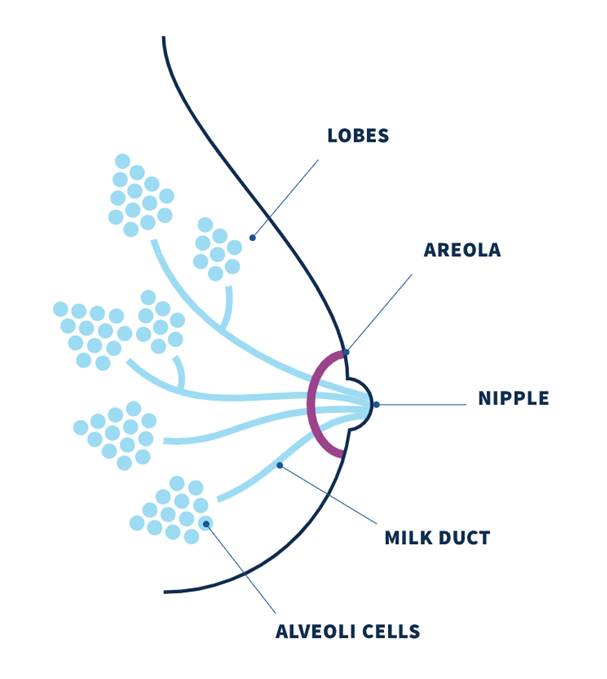
Inside your breast are milk making cells that form a sphere. These spheres are clustered together so I like to think of them as bunches of grapes with the stems representing the ducts that carry milk to the nipple.
Each grape is wrapped with muscle fibers. When your baby is feeding (or sometimes just when you think about your baby!) your oxytocin rises. Oxytocin is a hormone which plays a role in bonding, pleasure, and MER. It’s the same hormone that kicks starts uterine contractions during birth. The muscle fibers respond to oxytocin and squeeze milk down the ducts and out the nipple.
To have strong MER you need strong muscle contractions. Over the first 3 months, MER starts to chill out because those little squeezing muscles become less sensitive to it.
Oversupply
We actually just talked about oversupply. If you have an oversupply, when the muscles contract the milk making “grapes” are soo full that milk flows very quickly.
Ineffective Latch
Latch, or attachment to the breast, can be ineffective due to positioning, other medical conditions, tongue tie, or due to something else.

Hmmm, I think I know what’s going on. What do I do about it?
Make an appointment with your Lactation Consultant so they can give you personalized instruction and make a plan which will work for you!
All too often, the difficulty is with your baby and not with you. Your IBCLC can direct you to care which can include changing your feeding plan, adjusting your position, suck training exercises, working with a physical/occupational therapist, or SLP.
We are here to help!
❤ Megan

Many people think a plugged duct is caused by a backup of thickened milk but the plugging comes from outside the duct.
Our milk ducts carry milk from the milk making cells which are grouped together in alveoli. The alveoli are like little clusters of grapes which connect to the ducts. The ducts carry milk to the nipple openings.
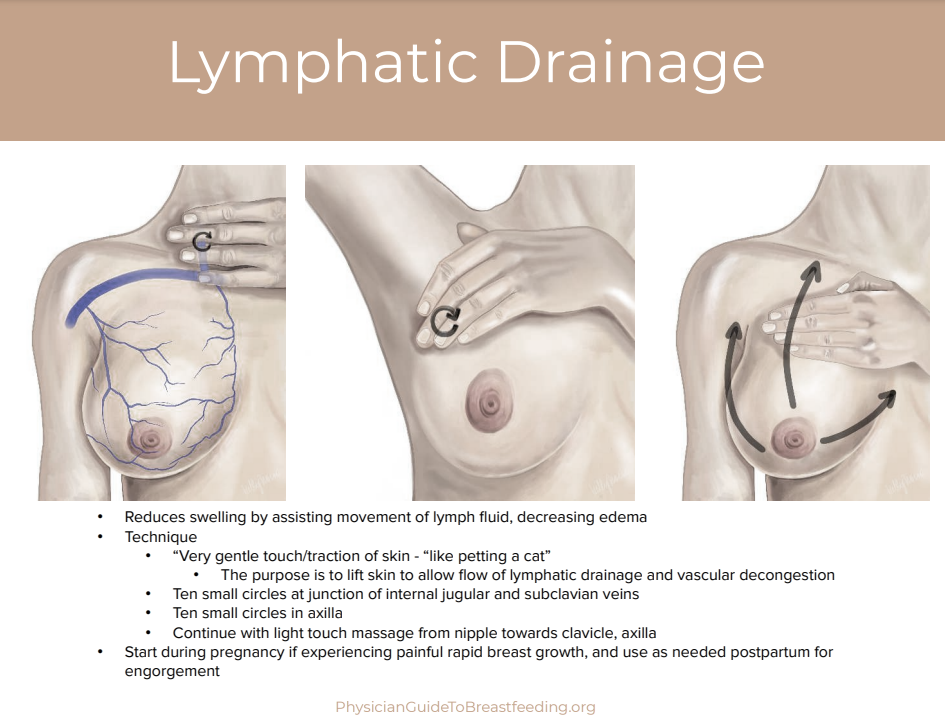
A breast “plug” represents an area of swelling in the breast and more accurately reflects lymphatic fluid congestion and dilated capillaries than a “plug of milk.” The plugging is caused by engorgement and congestion of fluid and blood vessels pressing in on the duct from outside which narrows the pathway.
Exclusive or excessive pumping, nipple shield use, oversupply, unresolved engorgement, inflammation, or subacute mastitis increases plugging.
To treat plugging, try the following:
This should resolve in 24hrs. If it does not, contact your provider and lactation consultant for guidance. Therapeutic ultrasound is very effective. Your doctor may prescribe a single dose of 10-30mg of Pseudoephedrine (Sudafed) which acts as a vasoconstricting agent (i.e. decreases blood flow) and may help with any pain.
Any plug or mass persisting for several days and not resolving with conservative interventions requires referral to a medical provider, who may obtain breast imaging to rule out galactocele and/or other mass.

Engorgement is common in the first week after delivery. Rather than a swelling caused by milk, it is an increase of fluid in the breast brought on by the same hormones which transition your colostrum to transitional and mature milk.
Extra fluids from labor (IV fluids) and some medications can increase this fluid retention. You might also notice it in your hands and ankles/feet. It tends to peak on day 5 after birth.
Sometimes, early mastitis is mistaken for engorgement. If you are still engorged after the first week, contact your Lactation Consultant to discuss what’s going on.
To reduce the engorgement very gentle massage can be helpful.
Wearing a soft and supportive garment like a bra without wires or a nursing tank is also helpful.
Frequent feeding will keep your milk flowing and contribute to breast softness. Aim for every 2 hrs, with rest in between. It’s important to let your breasts rest and the rest of you, too! We all need to sleep and rest to recover properly and ensure long-term milk production.
Excessive pumping will increase the engorgement. Instead try hand expression for a few minutes.
Diuretic foods (foods that help you urinate frequently) can also help. These can include melons, cucumber, lettuces and dark leafy greens. Avoid caffeine and salty foods.
If the feeling persists, the use of Tylenol and cold packs can provide some relief. Avoid excessive heat on the breast.
If not resolved with these measures contact your provider and lactation consultant. Therapeutic ultrasound can be helpful or your doctor may prescribe a single dose of Pseudoephedrine 10-30mg to relieve symptoms.
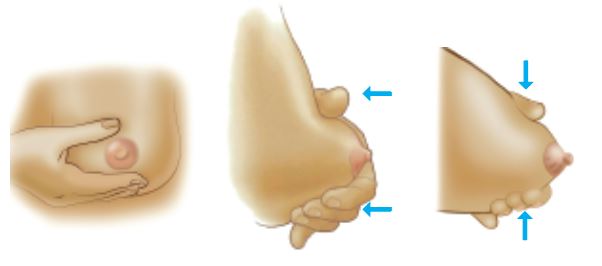
If your breasts are too full for baby to latch well, reverse pressure softening around the nipple may be helpful.

Hand expressing a little bit of milk may also be helpful.
Avoid: Pumping often (milk is not causing the fullness), firm or excessive massage, heat packs (increases inflammation).
You should feel better soon with these tips!
❤ Megan


Oversupply or hyperlactation can occur for a variety of reasons but is most common when early and excessive pumping, galactagogue (herbs and foods to promote lactation) use, and exclusive pumping.
You may notice engorgement past the first few weeks, pain, plugging, mastitis, or your baby may sputter or choke on your milk flow or even have a lot of spit up after feeds.
Once baby has reached two weeks of age, they only need 2-5oz per feeding (or about 1oz per hour). If you are finding that you need to pump after feeds or are producing significantly more than 5-6oz with exclusive pumping, you may have an oversupply.
An oversupply puts you at risk of an inflammatory breast condition called mastitis which can develop into an infection which ultimately will reduce your supply.
Work with your Lactation Consultant to address your oversupply. In the meantime, you can try a few things on your own.
❤ Megan

Mastitis is an inflammation in your breasts which may become an infection if not addressed. It affects about 1/3 of lactating parents but can be prevented and treated with quick resolution.

Mastitis is caused by inflammation and can be worsened by massage, excessive heat, overfeeding/overpumping.
If you’ve recently had a dose of antibiotics, your risk of developing mastitis is higher because a healthy balance of microbes throughout our body reduces inflammation and bacterial overgrowth. If left untreated, it can develop into an infection which will cause fever, fatigue, and overall body aches.
Mastitis may feel like a burning or hot sensation in your breast. It might start at the nipple and go deep into the breast. It’s more frequently felt in the lower parts of the breast. You may notice plugging or red areas in the breast. Early inflammation is sometimes mistaken for engorgement or plugged ducts.
For some parents, the feeling happens during milk ejection (letdown) and can feel like a burning or stinging sensation starting at the nipple and moving deeper into the breast.
Most commonly mastitis occurs during the first 2-4 weeks. Your risk of developing mastitis is higher if you have diabetes or if you have had antibiotics during or after delivery (ie, Group B Strep). It’s especially important to feed baby often and well in these situations.

Your milk is safe for baby when you have mastitis
Your Lactation Consultant can help you figure out how to
prevent mastitis from re-occurring.
Self-care can resolve the inflammation in most cases without the use of medication.
To treat mastitis, try the following:
Older recommendations included warm compresses, feeding and pumping very often, as well as vigorous massage. We now know this can increase symptoms.
Multiple studies have reported that probiotics (beneficial bacteria) are effective in treating infectious mastitis and also resulted in a lower occurrence of repeat mastitis compared to antibiotic treatment.
Call your doctor if you experience:
Fever over 101F
Flu-like aches
Nausea and chills
Pain and swelling in the breasts
Red, hot, tender area which is often wedge shaped
Red streaking toward the armpit
You should start to feel better in 8-24 hours. If you are not feeling better with self-care or you develop a fever, flu-like symptoms, or any signs of infection you will need to see your physician. Most people feel much better after 2 days but it’s important to take all 10-14 days of your medication or you may develop an abscess which requires surgical treatment. The most common antibiotics prescribed for mastitis are dicloxacillin or flucoxacillian.
Antibiotics can cause digestive symptoms so follow your doctor’s directions and taken your probiotic dose 2-4hrs after your medication.
Work with your Lactation Consultant to prevent mastitis from happening again.
If you get mastitis frequently or it’s always in the same area, your doctor may order an ultrasound to get more information.
❤ Megan Dunn, IBCLC
