Bodywork or manual therapy includes many types of hands-on treatments focused on supporting normal movement and function.
This can include chiropractic care, cranial sacral therapy, osteopathic manipulation, and many other therapies! When selecting a provider ask about them how often they care for infants and what additional training they have for working with babies.
Babies who experience a challenging birth – like a c-section, vacuum, or even just a not ideal position in the womb – often present with tension in their body which can impact their feeding, contentedness, sleep, and crying.
On the flip side, an infant with feeding problems can, over time, develop these same problems due to compensations.
What’s a compensation?
A compensation is what we do when the normal way of doing something isn’t working.
Twist your left ankle? Well, you might lean into using your right side a bit more until you heal.
It’s the same with our babies
If it’s not comfortable to move or feed in the normal way, they may develop compensations.
Okay, what’s the problem with that?
Compensations when used long term are dysfunctions.
Baby is using muscles which aren’t developed enough to work how they are using them. It also puts baby into a stressful state called sympathetic state.
This often means they cry more, have digestive problems are just generally not content. This is stressful for parents, too!
Bodywork and manual therapy for infants is incredibly gentle and works with their body to get back to balance. Gentle touch and massage can be beneficial for all babies!
And if your baby is having feeding problems which aren’t resolving with basic help or interventions, if your baby cries a lot, has sleep or nap difficulties, or it just doesn’t feel right…be sure to contact your provider and IBCLC for a referral to a skilled infant bodyworker. It may be just the thing your baby needs to feel better.
Manual therapies like chiropractic, osteopathic manipulation (these first 2 are most likely to be covered by your insurance), cranial sacral therapy (focuses on the head/neck/shoulders only), physiotherapy, and many more!
The practitioner and their skill set is an important factor in deciding which type to go with along with the areas your baby needs treated, your IBCLC or pediatrician should help you determine which will be right for your baby.
2. Oral motor exercises
These gentle exercises are meant to address compensations and work toward function. They are done in the mouth and on the face and may include other body movements. Unlike bodywork, these exercises are done daily by the parents as directed by your IBCLC. Some providers call this Suck Training.
3. Managing the feeding plan
This is evaluated and organized by your IBCLC. The feeding plan balances the need of the infant and parent and works toward feeding goals.
Your IBCLC will manage your feeding plan according to your goals and to get the bet outcomes for you. This can include counseling on pumping, feeding positions and techniques, supporting milk supply, and referring to other providers.
*these first 3 components are part of your pre and post release plan*
4. An effective release
Scissors or laser …it doesn’t matter as long as your provider is skilled and performs a full release to allow the tongue and/or other tissue to move normally. The release allows for movement while bodywork, oral motor training, and feeding plan management work together to get to normal function.
5. Wound care
Sometimes called stretches or exercises these are targeted on the site which was released (the diamond shape under the tongue). Wound care is necessary for posterior releases to prevent reattachment and aid in the tissue healing correctly.
Sometimes your provider will suggest oral motor exercises along with the wound care. Your IBCLC will suggest additional, customized oral motor training in addition to these.
Without all 5 components your baby may not achieve full functionality. Your IBCLC should be able to guide you through this process and make referrals to skilled providers as needed.
What to Expect After a Tongue Tie Release (Frenotomy)
When appropriate anesthetic is used, the procedure is generally not painful but it is irritating to be swaddled and have the mouth held open for the procedure. Your baby may be a little fussy after but can be soothed with skin-to-skin and a feeding.
Baby may initially feed very well but about 5-6 hours later they may be quite fussy and difficult to console. When adults get the procedure done, they report that they experience muscle fatigue which is quite uncomfortable. Try not to use a pacifier and instead to offer skin-to-skin and other forms of soothing. Smaller, closer spaced feeds may work better temporarily.
Work with baby’s skills and abilities. We aren’t trying to challenge their feeding during healing. Latch and hold your baby the way that works best for them.
Feeding starts to improve over time as the tongue strengthens and other muscles which have been compensating start to relax. The suck training exercises (oral motor work) recommended are very important in this process of “teaching” your baby how to use their newly released tongue and to address areas of tightness and weakness.
After about 4-5 days the wound will start to contract and feel tight again. Many parents worry that this is reattachment. Continuing your gentle wound care is important to keep these tissues soft.
Stretches should be done quickly and gently. I don’t recommend doing them before feeds to avoid associations with feeding. If you practice the stretches on yourself and your baby before the procedure it will increase your confidence and skill.
Effective and comfortable feeding requires a lot more than just a tongue which can fully move and function. It also requires that baby isn’t experiencing pain or discomfort anywhere else. Bodywork helps baby find full function through gentle manipulations. This can include pediatric chiropractic, osteopathic manipulation, cranial sacral therapy, or other types of bodywork. Ask your provider or IBCLC for referrals to providers who are experienced working with infants.
At home, you can support your baby with movement, massage, and at-home care like Tummy Time.
A visit with your IBCLC about 2-5 days after the procedure is important to check on the wound healing and to adjust your suck training and bodywork instructions.
March marks Plagiocephaly and Torticollis Awareness Month.
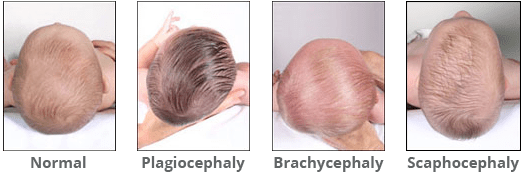
Plagiocephaly is when a baby develops a flat spot on one side or the back of the head. It happens when a baby sleeps in the same position most of the time or because of problems with the neck muscles that result in a head-turning preference.
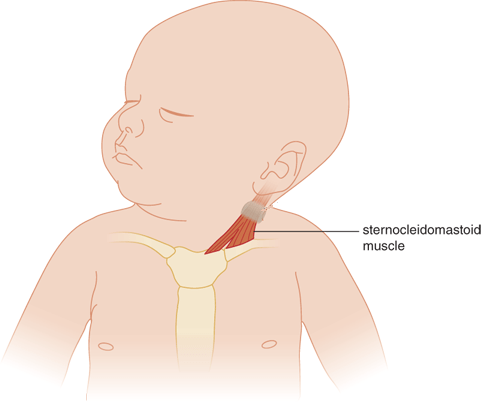
In babies, torticollis happens when the muscles that connect the breastbone and collarbone to the skull (sternocleidomastoid muscle) are shortened.
There are many reasons that babies can develop these conditions and none of them are your fault! In fact, plagiocephaly and torticollis are becoming increasingly common.
Here are some reasons your baby may have one or both of these conditions:
Being malpositioned in the uterus. A smaller parent may not have as much room for a larger baby which can put baby in the same position for days or even weeks before birth. This can occur with pelvic floor issues or with parents that have differing anatomy
Babies who sleep on their back for long stretches. While sleeping on the back is safest overall, if baby doesn’t move around a lot and sleeps looooong stretches it can increase flattening of the back of the head. These babies need lots of tummy time when awake!
Babies with reflux or torticollis may develop plagiocephaly on the side of the head. When we turn our head, it helps close off the esophagus during refluxing.
A baby who is best soothed in a swing or other baby-holding device. If your baby spends a lot of time in a swing, bouncy chair, or car seat it’s much more likely they will develop plagiocephaly.
The good news is that you can treat both of these conditions! Working with a pediatric PT is very helpful!
At home you can do fun activities with your baby to help them develop and improve.
Encourage baby to turn their head both directions by offering stimulation on the non-preferred side. Talk to them and sing songs to get baby to turn their head. Position baby for sleeping so they will turn to the non-preferred side toward you.
Babywearing is a great way to soothe baby and keep your hands free!
Cranial sacral therapy, OMT, and chiropractic can all be great options. Look for a provider that specializes in infants and ask your Pediatrician for recommendations.
With help and time, it will get better and you are likely to see big improvements in your baby’s feeding, too!
Does your baby gag, choke, and cough during feeding? Are they sputtering and tugging on your breast? Ever notice them clicking or leaking milk? What about gas…do they seem to have an awful of it?
There could be a number of things causing baby to struggle with feeding.
It could be a strong letdown (or as we call it in healthcare Milk Ejection Reflex – MER)
I could be an oversupply
It could be ineffective latch.
Let’s learn about the differences.
Strong MER Inside your breast are milk making cells that form a sphere. These spheres are clustered together so I like to think of them as bunches of grapes with the stems representing the ducts that carry milk to the nipple. Each grape is wrapped with muscle fibers. When your baby is feeding (or sometimes just when you think about your baby!) your oxytocin rises. Oxytocin is a hormone which plays a role in bonding, pleasure, and MER. It’s the same hormone that kicks starts uterine contractions during birth. The muscle fibers respond to oxytocin and squeeze milk down the ducts and out the nipple. To have strong MER you need strong muscle contractions. Over the first 3 months, MER starts to chill out because those little squeezing muscles become less sensitive to it.
Oversupply We actually just talked about oversupply. If you have an oversupply, when the muscles contract the milk making “grapes” are soo full that milk flows very quickly.
Ineffective Latch Latch, or attachment to the breast, can be ineffective due to positioning, other medical conditions, tongue tie, or due to something else.
Hmmm, I think I know what’s going on. What do I do about it?
Make an appointment with your Lactation Consultant so they can give you personalized instruction and make a plan which will work for you!
All too often, the difficulty is with your baby and not with you. Your IBCLC can direct you to care which can include changing your feeding plan, adjusting your position, suck training exercises, working with a physical/occupational therapist, or SLP.
Unfortunately, many parents experience nipple discomfort.
It’s not that breastfeeding causes this pain but other things can like a latch which isn’t deep enough, infant conditions like tongue tie, pumping (too much, wrong size flange…), or even some ointments and balms.
The best nipple ointments for soothing the skin or for use as a pumping lubricant don’t contain lanolin, coconut oil, or petroleum products. Try an organic product like Earth Mama,Bamboobies, or Motherlove. Other ingredients may cause an allergic reaction or irritation (dermatitis).
There is a prescription ointment called APNO (All Purpose Nipple Ointment) which should be used only as indicated as it’s an anti-bacterial, anti-fungal, and steroidal compound. Nipple pain is very rarely caused by fungus/yeast but anti-fungal medications can actually increase pain.
Care for the nipple like any other skin on your body… Wash once per day with mild, scent free soap. Keep the skin clean and dry.
If there is tissue damage: Lubricate with a moisturizing balm (see above) or try Medi-honey (irradiated, medical grade honey and many nipple wounds respond well to treatment).
Hydrogel pads (changed daily) protect the wound from irritation and keeps the site clean. You can use this with your nipple balm. Expect healing to take at least 1 week.
Avoid:
Nipple shields. Despite the name, these products do not shield your nipple and can cause irritation. They also increase risk of low supply, engorgement, and mastitis.
Gentian violet can cause tissue ulceration. It’s often used to combat yeast which is very unlikely to infect the nipple.
Epsom salt soaks, tea bags, or excessive use of moist compress can break down skin.
Breast shells can cause swelling in the areola and often increase pain.
Using a hair dryer which will dry out the skin.
Nipple bleb. A bleb can look like a little blister which may be white or yellow on the nipple. Blebs show up when there is deeper inflammation and bacterial imbalance. Treat the underlying mastitis (inflammation) and the bleb will resolve. If you have a bleb, let your Lactation Consultant know. Do not try to squeeze or pop the bleb as that will open the skin for infection.
Vasospasm. If your nipples turn colors after feeding (white, purple, or blue) you may be experiencing vasospasm. This is caused by a constriction of blood flow from nipple damage, poor latch, or topical anti-fungals. Fixing the cause stops the vasospasm.
Alexa Blake, CCC-SLP, has been working for the last two and a half years to develop andgrow an infant feeding and swallowing program that serves Linn and Benton counties. She works at Samaritan Lebanon Community Hospital and considers it her passion project to serve these little warrior humans and their parents, optimizing feeding safety and function and meeting the goals of the family. She works with infants who have feeding difficulty from prematurity, tongue tie, torticollis, and general oral motor weakness, using a variety of oral motor and sensory based techniques to meet the unique needs of each patient. The thing that makes her work even more special to her, though, is her own experience with nursing difficulty with her son who was born with a tongue tie.
Here’s her perspective:
I began working with infants prior to having my own child, and I really enjoyed it. It was a unique challenge and very different from any other kind of patient population I’d worked with previously. So when it came time to feed my own child, I figured I had a leg up on how to make it successful for both of us. Once he arrived however, it was a whole different ball game.
My son was born health and happy at 39 weeks, and I weathered my birth experience just fine. All things considered, we were off to a great start. The first time he nursed, just about half an hour after he came in to this world, he ate for a full 80 minutes and I was proud of this accomplishment, taking that as a sign he was hungry and ready to eat. Nursing did not feel great, but compared to childbirth it was nominal pain. The discomfort persisted and worsened over the first several days and my nipples became bruised, chapped, bloodied, and so on. It got to the point that I could not nurse him without tears streaming down my face from the pain. My son was colicky and screamed at all the things everyone said would make him happy (baby swing, I’m looking at you), had frequent and aggressive spit up out his nose, gas, and was a sleepy eater. I did not know how to fix our feeding difficulties or any of the other resultant challenges we were having.
Teddy and Alexa
I went to three different lactation consultants over the next week to try and solve my nursing pain, and each of them hinted at a posterior tongue tie. Initially, I was offended. I was a new feeding therapist, how could my child have a tongue tie? And even more, how could I not have been the one to figure it out? I had been given holding techniques to try, nipple shiels, creams, etc. to address our feeding struggles and nothing was working. I felt scared and frustrated. I wanted to nurse so badly and felt I would’ve failed my son to do otherwise.
At 11 days old, I took my son to an ENT who laser beamed my son’s tongue to release the tethered tissue. I thought that would be the end of it and things would get better. I was instructed to stretch his wound 6 times a day for a whole month to help it heal properly. To me, in the throws of a post-partum hormone crash with a colicky baby, those stretches were pure torture for both myself and my newborn son. I loathed them, and yet, I was fearful that if I did not do them it would all be for naught.
It was at this point that I asked for help from anyone and everyone I could think of who would help my baby’s mouth and keep us nursing. We went to OMT, we had a home visit from my PT superwoman coworker Patsy Yelsa, I consulted fellow feeding therapists on what an SLP could do, I saw lactation. It was my mission to turn this experience around. And slowly but surely, we did just that. I found a combination of frenotomy stretches and oral motor exercises that allowed my son to do rehab without causing me to feel I was hurting him. We addressed my baby’s whole body experience with his tongue tie, not just his mouth. We worked hard on tummy time, proper positioning, and latch. My nursing pain subsided and my supply stabilized. It took the first 8 weeks of his life before I felt like we both knew what we were doing. It took a whole team of people and professionals help us be successful. He continued to grow, his colic subsided, his reflux improved, and I felt capable of sustaining him with my own milk.
Our nursing journey concluded 15 months after he was born, slowly and on both our terms, when he was ready to move on to bigger and better toddler things. The experience of nursing my child has been one of the greatest treasures I’ve ever had and I’m so thankful we were able to continue for as long as worked for both of us.
My experience with tongue tie has also been invaluable for my clinical practice as I have really been able to incorporate that compassion and first-hand understanding of what it feels like to be a mom with a baby who just can’t eat properly into my therapy. I know better now what is reasonable to ask of new mom’s/parents, I know what consistency and determination can do. I also know that my journey is not everyone’s journey and that finding a way to help moms’ meet their goals for feeding their children must be central to any therapy I do. I love my job, I love working with babies, and I am so privileged to get to walk alongside families on their feeding journeys.
Lots of parents are surprised to find out their baby has ankyloglossia (tongue tie) and that such a tiny piece of tight tissue under the tongue is causing so many feeding problems!
Luckily, it a simple procedure to release the tongue and get on our way to easier feeding!
In my experience providing care for babies with tongue tie, doing just “the snip” isn’t enough to get full results. If we think about how baby has never had full range of motion with the tongue it makes sense that they will need time and help to get to normal movement.
Of course, working with a tongue tie-saavy Lactation Consultant and your provider is key but there are also things you can do at home!
Top 5 At-Home Tongue Tie Care
Tummy time
You may already be doing this with your baby but there are some modifications which may improve outcomes for tongue tied babies. Try rolling up a blanket or using your nursing pillow under their chest. This can be more comfortable for some babies and make the whole process more enjoyable.
My favorite recommendations come from the Tummy Time Method which has parent handouts and lots of suggestions for tongue tie specifically
Guppy Hold
The Guppy Hold is great for stretching tight neck muscles and it’s very easy to do! Babies love it. Check out this video for more info
Play with baby’s mouth!
Try running a clean finger from one side of their gums to the other. They will “chase” you with their tongue. This is a fun stretch which encourages good movement.
You can also insert a clean pinky finger, nail side down, once baby starts sucking pull gently. You are just adding a little resistance for baby to help strengthen their suck.
When I’m doing these games, I like to sing a little made up song to engage baby and reinforce that what we are doing is happy playtime!
Give baby options
Move around where you place baby during the day when they aren’t snuggling in your arms. Switch up how they are faced at bedtime. Baby will naturally turn their head toward you so by switching it up, they will take turns looking both ways.
The same goes for feeding. Breastfeeding on both sides is great and bottle feeding on both sides is great, too!
Massage
Massage and gentle touch is beneficial for many conditions, tongue tie included. This video has a great demonstration of massage parents can do on their own.
The biggest thing, is to have patience and keep working with your experienced tongue tie-saavy Lactation Consultant for continued help.


















{kind=link}
{kind=link}
{kind=link}
{kind=link}