





As many as 1 in 7 parents experience chronic low milk supply.
An estimated 5-15% of lactating parents experience CLMS (chronic low milk supply).
CLMS is associated with many common metabolic and endocrine conditions like:
Up to 20% of lactating parents may have PCOS

Many parents don’t know why they experience CLMS. There are significant Mental Health impacts from CLMS.
Experiencing CLMS may compound trauma and feelings of inadequacy from infertility, pregnancy, or birth challenges.
Connecting with other parents who have similar experiences and working with your IBCLC to make feeding comfortable and enjoyable can help.
Resources for support:
Wellmama http://www.wellmama.net 541-231-4343
Hope for Mothers Albany 541-812-4475 Lebanon 541-451-7872
Low Milk Supply Foundation https://lowmilksupply.org/
❤ Megan


Does your baby gag, choke, and cough during feeding? Are they sputtering and tugging on your breast? Ever notice them clicking or leaking milk? What about gas…do they seem to have an awful of it?
There could be a number of things causing baby to struggle with feeding.
Let’s learn about the differences.

Strong MER
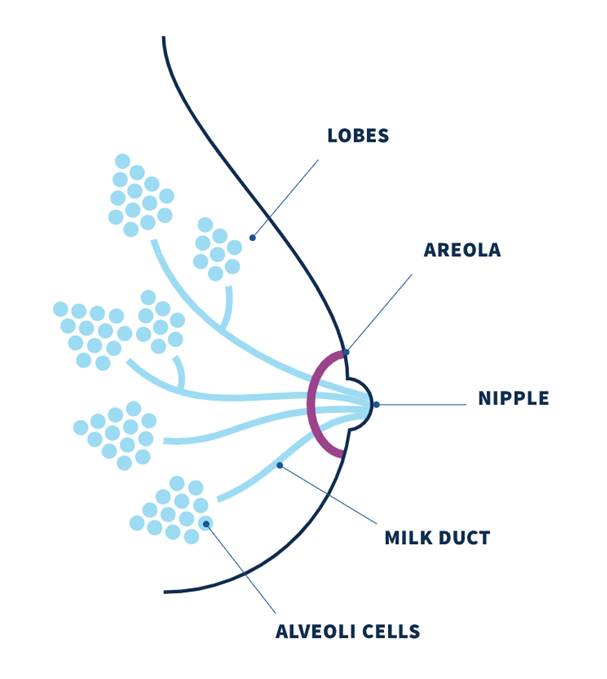
Inside your breast are milk making cells that form a sphere. These spheres are clustered together so I like to think of them as bunches of grapes with the stems representing the ducts that carry milk to the nipple.
Each grape is wrapped with muscle fibers. When your baby is feeding (or sometimes just when you think about your baby!) your oxytocin rises. Oxytocin is a hormone which plays a role in bonding, pleasure, and MER. It’s the same hormone that kicks starts uterine contractions during birth. The muscle fibers respond to oxytocin and squeeze milk down the ducts and out the nipple.
To have strong MER you need strong muscle contractions. Over the first 3 months, MER starts to chill out because those little squeezing muscles become less sensitive to it.
Oversupply
We actually just talked about oversupply. If you have an oversupply, when the muscles contract the milk making “grapes” are soo full that milk flows very quickly.
Ineffective Latch
Latch, or attachment to the breast, can be ineffective due to positioning, other medical conditions, tongue tie, or due to something else.

Hmmm, I think I know what’s going on. What do I do about it?
Make an appointment with your Lactation Consultant so they can give you personalized instruction and make a plan which will work for you!
All too often, the difficulty is with your baby and not with you. Your IBCLC can direct you to care which can include changing your feeding plan, adjusting your position, suck training exercises, working with a physical/occupational therapist, or SLP.
We are here to help!
❤ Megan

Many people think a plugged duct is caused by a backup of thickened milk but the plugging comes from outside the duct.
Our milk ducts carry milk from the milk making cells which are grouped together in alveoli. The alveoli are like little clusters of grapes which connect to the ducts. The ducts carry milk to the nipple openings.
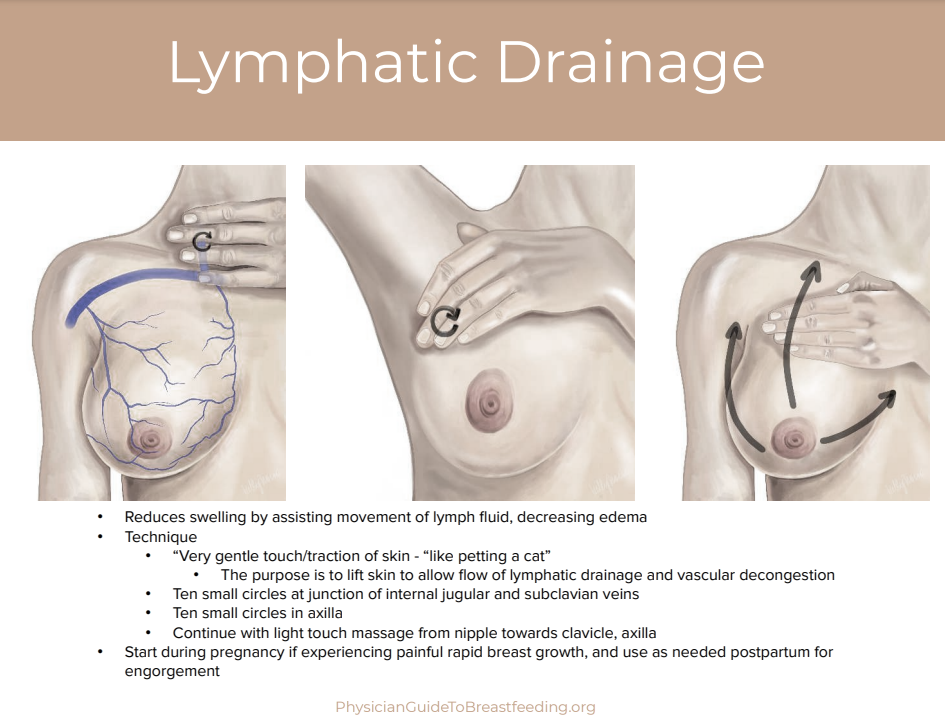
A breast “plug” represents an area of swelling in the breast and more accurately reflects lymphatic fluid congestion and dilated capillaries than a “plug of milk.” The plugging is caused by engorgement and congestion of fluid and blood vessels pressing in on the duct from outside which narrows the pathway.
Exclusive or excessive pumping, nipple shield use, oversupply, unresolved engorgement, inflammation, or subacute mastitis increases plugging.
To treat plugging, try the following:
This should resolve in 24hrs. If it does not, contact your provider and lactation consultant for guidance. Therapeutic ultrasound is very effective. Your doctor may prescribe a single dose of 10-30mg of Pseudoephedrine (Sudafed) which acts as a vasoconstricting agent (i.e. decreases blood flow) and may help with any pain.
Any plug or mass persisting for several days and not resolving with conservative interventions requires referral to a medical provider, who may obtain breast imaging to rule out galactocele and/or other mass.

Engorgement is common in the first week after delivery. Rather than a swelling caused by milk, it is an increase of fluid in the breast brought on by the same hormones which transition your colostrum to transitional and mature milk.
Extra fluids from labor (IV fluids) and some medications can increase this fluid retention. You might also notice it in your hands and ankles/feet. It tends to peak on day 5 after birth.
Sometimes, early mastitis is mistaken for engorgement. If you are still engorged after the first week, contact your Lactation Consultant to discuss what’s going on.
To reduce the engorgement very gentle massage can be helpful.
Wearing a soft and supportive garment like a bra without wires or a nursing tank is also helpful.
Frequent feeding will keep your milk flowing and contribute to breast softness. Aim for every 2 hrs, with rest in between. It’s important to let your breasts rest and the rest of you, too! We all need to sleep and rest to recover properly and ensure long-term milk production.
Excessive pumping will increase the engorgement. Instead try hand expression for a few minutes.
Diuretic foods (foods that help you urinate frequently) can also help. These can include melons, cucumber, lettuces and dark leafy greens. Avoid caffeine and salty foods.
If the feeling persists, the use of Tylenol and cold packs can provide some relief. Avoid excessive heat on the breast.
If not resolved with these measures contact your provider and lactation consultant. Therapeutic ultrasound can be helpful or your doctor may prescribe a single dose of Pseudoephedrine 10-30mg to relieve symptoms.
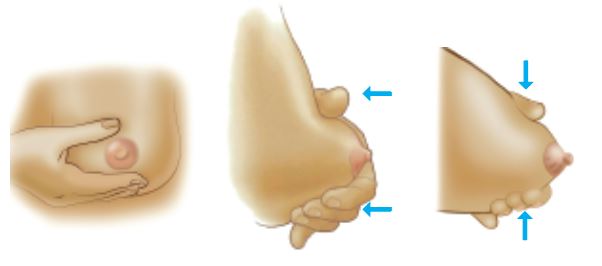
If your breasts are too full for baby to latch well, reverse pressure softening around the nipple may be helpful.

Hand expressing a little bit of milk may also be helpful.
Avoid: Pumping often (milk is not causing the fullness), firm or excessive massage, heat packs (increases inflammation).
You should feel better soon with these tips!
❤ Megan


Oversupply or hyperlactation can occur for a variety of reasons but is most common when early and excessive pumping, galactagogue (herbs and foods to promote lactation) use, and exclusive pumping.
You may notice engorgement past the first few weeks, pain, plugging, mastitis, or your baby may sputter or choke on your milk flow or even have a lot of spit up after feeds.
Once baby has reached two weeks of age, they only need 2-5oz per feeding (or about 1oz per hour). If you are finding that you need to pump after feeds or are producing significantly more than 5-6oz with exclusive pumping, you may have an oversupply.
An oversupply puts you at risk of an inflammatory breast condition called mastitis which can develop into an infection which ultimately will reduce your supply.
Work with your Lactation Consultant to address your oversupply. In the meantime, you can try a few things on your own.
❤ Megan

Over the last few years it seems like everyone is jumping on the lactation cookie trend. New pre-made products have been popping up online and in stores all with strong claims about how they will help.
I love a cookie as much as any one (warm oatmeal or spicy snickerdoodle…yes, please!) but I don’t recommend them as a Lactation Consultant for milk production.

This is for a few reasons. I have noticed that lots of my patients come to me already trying to take herbs and alter their diet to support milk supply. They invest hundreds of dollars sometimes without really knowing the exact cause of their milk supply problems. Often the issue is low milk supply perception without an actual issue but when there is a problem, it needs to be addressed by a medical provider who can investigate the source and give you personalized recommendations.
Different problems need different solutions.
A thorough assessment and history taking can often pinpoint the problem and then we can give you the right “medicine” for what’s really going on. Otherwise, it’s like throwing a dart in the dark. It might hit the target, it might get close, but it’s probably just a random shot.
Milk supply is governed by milk removal. When we take supplements to boost our milk supply there may be some effect but it might also temporarily boost our supply without setting us up for good long term habits. At the beginning, prolactin hormone brings in our supply and transitions milk from colostrum to mature milk. Oxytocin hormone is the main reason that milk sprays and drips out. Over time, our breasts become less sensitive to these hormones and what we need for continued supply is a baby who can breastfeed well!
Which brings us to the next issue. If we take herbs or eat cookies that artificially boost our supply it can mask baby feeding problems. If your baby’s suck is weak or uncoordinated, I want to know that right away and get you on the path to healing! We can work with suck training, a physical therapist, or occupational therapist to make sure your baby is thriving. We don’t want to miss those early signs .
Homemade baked goods are about the most delicious thing I can think of but sometimes the ingredients might actually lower supply. Many recipes call for a fair amount of sugar so if the milk supply problem is created by insulin resistance it won’t be supportive. Some of the other herbal ingredients might also lower supply. Some of the most common herbal ingredients for milk supply are not compatible with the medical conditions which are most likely to impact supply!
And lastly, I think it’s important to consider that we do not need to eat a special or different diet while breastfeeding. Our milk can be plentiful and super healthy following standard recommendations for adults. Our diets may need to be altered for medical reasons and if so, ask your provider to help you come up with a plan. Many of the ingredients in lactation cookies are expensive and hard to find. I’d rather see you snuggled up in bed nibbling on a grocery store oatmeal cookie than driving from store to store for specialty ingredients.
As always, take what works for you and leave the rest behind. Know that this Lactation Consultant won’t judge or tell you what to do. We are here to support you. And if you sister or kind neighbor brings you lactation cookies, feel free to eat them if they work for you and you want to. Just know you don’t *have* to eat them to make lots of milk.
If you are experiencing low milk supply check out our local Lactation Consultants for support and up-to-date information.
<3Megan Dunn, IBCLC


This builds up hormone receptors which help you to make the most milk! It also gets you familiar with the technique which is super helpful to do at least 5 times a day after birth (for the first 2 weeks). If you hand express into a clean container you can store the colostrum (early milk) in the freezer and bring it with you in case your baby needs a supplement after birth.
2. Golden Hour
Hold your baby skin-to-skin after delivery until baby has had their first meal.
It takes time to adjust to the outside world! It’s so bright and loud and cold! Let baby find their way to the breast and attach on their own –they can do it if we give them time.
Our bodies are also primed from labor to transfer the most colostrum in the first few hours, so make the most of it!
3. Have a Nursing Marathon for 3 days after birth
Feed often (at least 10 times per 24 hours) especially when baby is awake and calm, hold baby skin-to-skin as much as you can, and do hand expression at least 5 times per day after feeds. This tells your body to make lots of milk and helps prevents swelling (which is also called engorgement).
Keeping baby close by will help everyone rest and recover. Snuggling baby often also reduces crying!
Megan Dunn, IBCLC
